
With the inauguration of Donald Trump as US President and the UK Supreme Court decision on Brexit, the crisis in our National Health Service seems to have fallen to the back of the news agenda, at least temporarily. Yet, there is a close connection between these issues.
In the post Brexit world, we are about to embark on trade negotiations with a US administration committed to dismantling affordable healthcare provision for the poorest people in US society. This agenda arises from a deep Republican belief in the private sector’s role in healthcare even if that means some must go without life-saving treatment. This is the polar opposite of the deeply held and almost universally shared UK belief in health as a public service, funded through fair taxation and delivered equally to every citizen free of charge.
I am very much afraid that this difference of approach will play out in the forthcoming trade negotiations as the US seeks access for their businesses to the supply of goods and services to the NHS. This doesn’t just mean giving NHS purchasers the option of buying drugs from US companies. It could mean they are forced to open every aspect of NHS provision to competitive tendering (and US companies could sue for loss of profits if they don’t) leading to an NHS which could quickly become completely dependent on US big business, and the effective and irreversible privatisation and foreign ownership of our health service.Not only would we still have to find the money to pay for healthcare, we would also have to pay for the profit margin that would give a return to American businesses.
This concern is one of the reasons the secretive TTIP trade negotiations between the US and the EU have so far failed to achieve agreement. If we are negotiating on our own, without the collective strength of the EU around us, will we be able to reach an agreement that protects our health service, or will our Government be willing to put the NHS up for sale in return for wider access to the US market? But, in voting to leave the EU, the British people were voting in favour of a publicly funded NHS (remember the £350m a week promise) so Brexit gives the Government no mandate for selling our NHS off to US business and we should campaign hard to ensure that doesn’t happen.
Leave campaigners during the referendum campaign argued that leaving was a means of saving the NHS from the marketisation that would inevitably result from TTIP (http://www.telegraph.co.uk/news/2016/04/06/nhs-would-be-completely-unrecognisable-within-years-if-uk-remain/) so let’s hope all the Brexiteers, in Government and outside it, will now argue against replicating the worst of TTIP in any bilateral negotiations between the UK and the US.
A highly critical article on TTIP in the Independent newspaper (http://www.independent.co.uk/voices/comment/what-is-ttip-and-six-reasons-why-the-answer-should-scare-you-9779688.html) states:
One of the main aims of TTIP is to open up Europe’s public health, education and water services to US companies. This could essentially mean the privatisation of the NHS.
The European Commission has claimed that public services will be kept out of TTIP. However, according to the Huffington Post, the UK Trade Minister Lord Livingston has admitted that talks about the NHS were still on the table.”
Personally, I am very proud of the NHS and the dedicated public servants who do their best for us, the patients, under increasingly severe financial pressures. Brexit is already going to make this more challenging if the Government restricts immigration of the people we depend on for our health service. At the same time the NHS is facing a financial squeeze as demand grows faster than funding. Together with the potential pressures for privatisation, this amounts to a triple whammy for the NHS.
The results of the current pressures are clear for all to see even before the impact of Brexit and trade deals are added. Local GP surgeries especially in rural areas are struggling to fill vacancies and early appointments are hard to come by, contributing to increasing pressure on hospital emergency departments. That pressure is exacerbated by the crisis in care provision which is blocking beds in hospitals as patients have nowhere safe and secure to go if discharged. In the face of these pressures, the Government has chosen to prioritise a seven day service without providing any extra resources and when the NHS is struggling to provide its current level of service. I would love to see healthcare more readily available whatever the day of the week, but this can’t be achieved simply by demanding that hard pressed staff work even harder with no more money in the budgets of their practices and hospitals. Instead of valuing, praising and supporting the young doctors who already work long hours caring for us, the Government chose to pick an unnecessary fight with them.
Mrs May’s speech setting out her approach to the Brexit negotiations contains a further potential threat to the NHS. She has set out the possibility that the UK could reduce corporate tax rates still further in order to compete with the EU in attracting inward investment. She said:
“we would have the freedom to set the competitive tax rates and embrace the policies that would attract the biggest companies and investment”
This would mean further reducing tax revenues which we need to fund public services, especially the NHS and social care. And it probably wouldn’t work as it could set off a competitive lowering of tax rates, when what is needed is precisely the opposite – co-ordinated international agreement to avoid such competition and ensure that companies pay what is needed to ensure services can be maintained. Just as people didn’t vote Brexit to privatise the NHS, neither did they vote Brexit for lower taxes on corporate profits.
The NHS is a shining example of Universal Health Coverage (UHC) which is now becoming a globally recognised model for the development of health systems around the world, including in developing countries. Here’s what the World Health Organisations says about UHC (http://www.who.int/mediacentre/factsheets/fs395/en/):
UHC means that all individuals and communities receive the health services they need without suffering financial hardship. It includes the full spectrum of essential, quality health services, from health promotion to prevention, treatment, rehabilitation, and palliative care.
UHC enables everyone to access the services that address the most important causes of disease and death, and ensures that the quality of those services is good enough to improve the health of the people who receive them.
Protecting people from the financial consequences of paying for health services out of their own pockets reduces the risk that people will be pushed into poverty because unexpected illness requires them to use up their life savings, sell assets, or borrow – destroying their futures and often those of their children”.
All UN Member States have agreed to try to achieve Universal Health Coverage (UHC) by 2030, as part of the Sustainable Development Goals. We have one of the most advanced and effective Universal Health Coverage systems in the world. This is what others aspire to and the world community has agreed is a global priority. Now is not the time for us to compromise on that achievement by cutting immigration access for the medical personnel we need, encouraging privatisation through open access to US companies under a UK/US trade deal, forcing hard pressed NHS staff to work longer hours under new contracts with no additional funding, or cutting the tax revenues we need to meet the growing demands of a longer-lived population.
During the recent spate of coverage of deaths in hospital corridors I was saddened to hear politicians from most parties using the easy line that “it isn’t just about money” or “we won’t solve the NHS’s problems just by throwing more money at them”. The reality is that the NHS is incredibly efficient and provides a fantastic service but when social care budgets are being cut, people are living longer, and new valuable (but expensive) treatments are becoming available, there simply isn’t enough money to enable the doctors, nurses and managers to deliver the service people need. Money is never the only issue, but in this case, it really is the main issue and it needs to be addressed – and with urgency. Yet in fact the Government’s funding plans show almost no real terms additional funding for the NHS in the coming years (https://www.kingsfund.org.uk/projects/nhs-in-a-nutshell/nhs-budget):

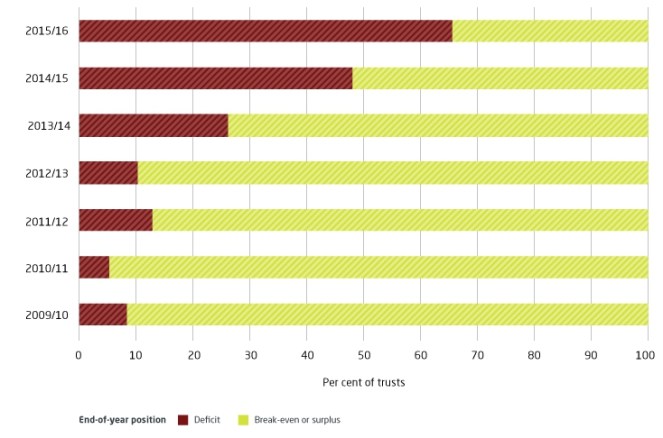
Already most NHS providers and commissioners are unable to operate within the budgets they have, ending 2015/16 with a combined deficit of £1.85 billion – the largest aggregate deficit in NHS history. (https://www.kingsfund.org.uk/projects/nhs-in-a-nutshell/trusts-deficit):
As a proportion of GDP NHS funding will fall to 6.6 per cent by 2020/21 compared to 7.3 per cent in 2014/15. But, if spending kept pace with growth in the economy, by 2020/21 the UK NHS would be spending £16 billion more than is currently planned. That is the minimum gap that needs to be filled. We are now 13th out of the original 15 EU countries in overall health spending as a proportion of GDP (https://www.kingsfund.org.uk/blog/2016/01/how-does-nhs-spending-compare-health-spending-internationally).
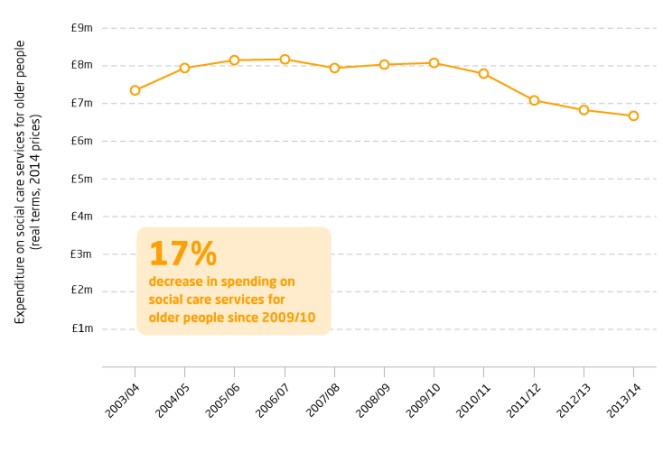
Meanwhile social care spending decreased 17% between 2009/10 and 2013/14 (https://www.kingsfund.org.uk/projects/nhs-in-a-nutshell/spending-social-care-older-people):
And the number of hospital beds has declined by more than 50% since the late 1980s (https://www.kingsfund.org.uk/projects/nhs-in-a-nutshell/hospital-beds). Much of this is to do with improvements in treatment allowing people to be treated out of hospital, but perhaps it also explains why it often seems so difficult to find beds when they are desperately needed:

So if we agree (as most people in the UK do) that the NHS needs more money, where should it come from? I am frustrated at hearing even relatively progressive commentators who should know better defaulting to the overseas aid budget. Health is the largest theme in UK bilateral aid and makes up a significant part of multilateral and humanitarian flows. Assistance for health includes, for example, the Ebola response, health prevention through water, sanitation and hygiene programmes and support for The Global Fund to Fight AIDS, TB and Malaria, and the Global Alliance for Vaccines and Immunisation. Taking money from the aid programme to support our NHS would mean enhancing our own health, in one of the world’s wealthiest countries, at the expense of the health of the world’s poorest people. And, as in the case of Ebola, that can also have a direct impact here as well – a world in which more children die unnecessarily of preventable diseases is not in our interests and it is not a moral choice. And even the entire UK aid budget is significantly less than even the minimum hole in the NHS budget. The money must be found elsewhere.

There are of course other options in terms of reprioritising expenditure, not least the £200bn or so likely to be spent on the trident nuclear weapon system over its lifetime. But the real answer must lie in increasing the Government’s tax revenue, particularly that gathered from the extremely wealthy in our very unequal society.
Opinion polls show that extra taxation is the most popular option to address the funding crisis which is almost universally recognised to exist. Other options such as payment for services or means testing NHS access gained far less public support, and those who said they were unwilling to pay more were a minority (https://www.theguardian.com/society/2014/aug/15/voters-tax-fund-nhs-poll) ( http://www.pharmatimes.com/news/42_of_patients_willing_to_pay_more_tax_for_nhs_1052762) . If the question were rephrased to ask whether big companies and top earners should pay more towards the health of everyone, I’m confident there would be widespread public support.
Media coverage of the impact on individual patients of denial of expensive cancer drugs demonstrate that there is little support for more stringent rationing of access to treatment. The NHS is already tasked with the near-impossible requirement to find £22bn in efficiency savings so more of that is not the answer. The other argument often heard is that there are too many managers and money should be spent on the front line. But no-one wants a badly managed NHS, or one in which management tasks have to be done by doctors, taking them away from patients. According to the Kings Fund (https://www.kingsfund.org.uk/topics/nhs-reform/mythbusters/nhs-managers), in 2009 managers made up 3.7% of the NHS workforce, compared to 15.4% in the whole 2010 UK workforce. That means each manager is responsible for an average of 27 staff. The Kings Fund concluded that the assertion that the NHS is over-managed is a myth:

Most of us know from our daily experience that NHS staff are generally amazing, dedicated and hard-working professionals; that many of them are immigrants who we need and welcome; that there are too few of them; that the NHS is in a financial crisis; and that we value, and wish to retain, a genuinely universal health system that is free and accessible to all.
If all that is true, as I firmly believe, then we have to find a way to solve the financial squeeze. It would be wrong to do so at the expense of the health of the poorest people on the planet, and cutting managers and improving efficiency are measures that have already been pushed to the limit or beyond. There is in the end only one serious option: the Government will have to raise the tax revenue to invest the additional funds our NHS so desperately needs. We should find the money to ensure that health services in the UK get at least the same share of GDP as in comparable EU countries. We should not be reducing taxes on the richest people and companies, but increasing them. And if ordinary standard rate taxpayers need to pay a little more then that still has broad public support relative to all other options. It is time our politicians had the courage to say so, instead of resorting to platitudes about managers, efficiencies, or the aid budget. Now is the time for them to be leaders, take responsibility and take the only steps that will ensure the continuation of the brilliant publicly funded, free health service of which we are all rightly proud and supportive.

Maybe we must say: Saving Mexico from Trump too? (Do you remember when you asked me about NAFTA time ago?..). Who do you think will pay for the wall? ( I think, we won´t, of course!, LOL..).
Read this interesting article:
http://www.forbes.com/sites/stuartanderson/2017/01/26/now-americans-not-mexico-would-pay-for-the-wall/#4581c0d151f0
Have a great weekend.
LikeLiked by 1 person